Hip and Groin pain

Anterior hip and groin pain could be due to a number of different reasons. But let’s talk about intraarticular hip pain.

▶️ Intra-articular hip pathology refers to pain and pathology within the hip joint
▶️ It typically presents as deep pain in the anterior hip and groin region and can also present as buttock pain
▶️ Common symptoms associated with hip flexion and rotation-based movement / activities
The Zurich consensus in 2018 classified hip related pain in young and middle-aged active adults into 3 categories:
1️⃣ FAI syndrome
2️⃣ Acetabular dysplasia and / or Hip instability
3️⃣ Other conditions without bony morphology causing hip pain
▶️ Chondral, labral and ligamentum teres conditions
Let’s take a dive into Femoroacetabular impingement (FAI)…
The Medical Subject Heading’s Thesaurus definition of FAI (Sankar et al. 2013)
This definition contains five essential elements:
1️⃣ Abnormal morphology of the femur and/or acetabulum,
2️⃣ Abnormal contact between these two structures,
3️⃣ Especially vigorous supraphysiologic motion that results in such abnormal contact and collision,
4️⃣ Repetitive motion resulting in the continuous insult, and
5️⃣ The presence of soft-tissue damage.
FAI is a motion-related or position-related pain in the hip or groin.
👉 More common in males affects approx. 15-25% males and 5-15% females (Argricola R, 2013)
👉 Pain is most likely due to an overload of acetabularlabrum and intra-articularchordal surfaces.
2 types of FAI
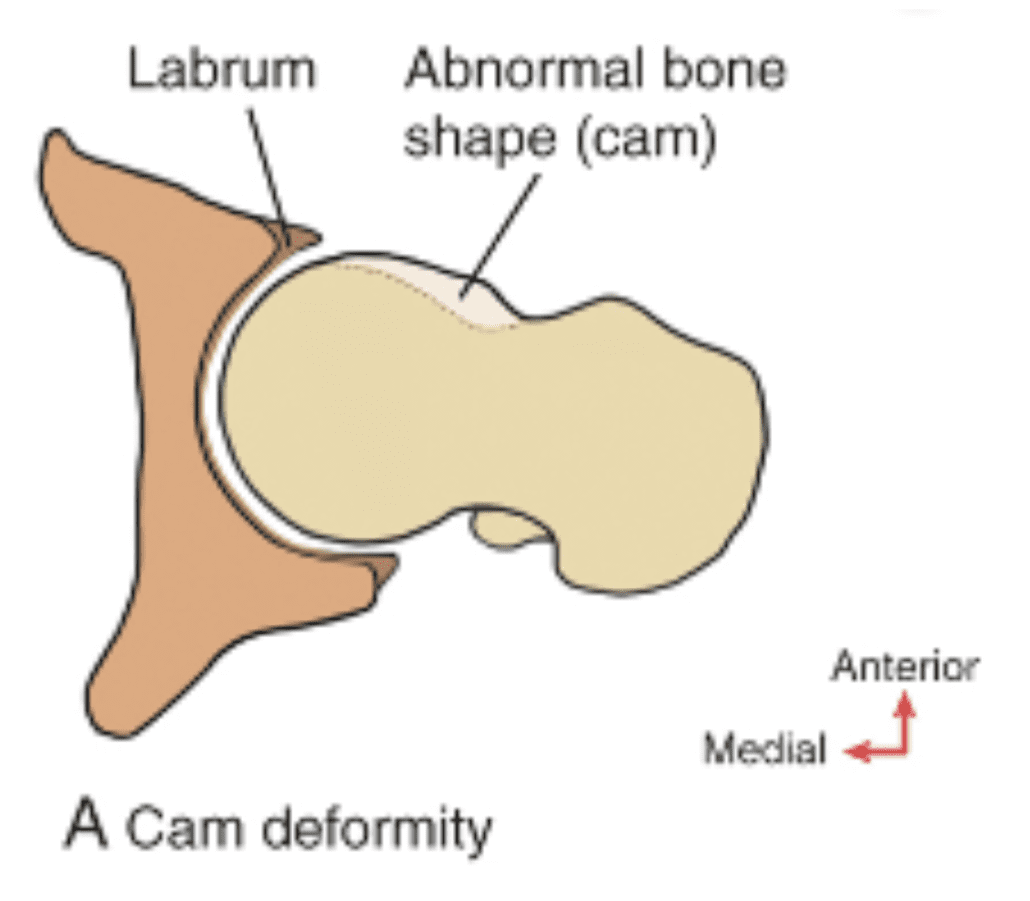
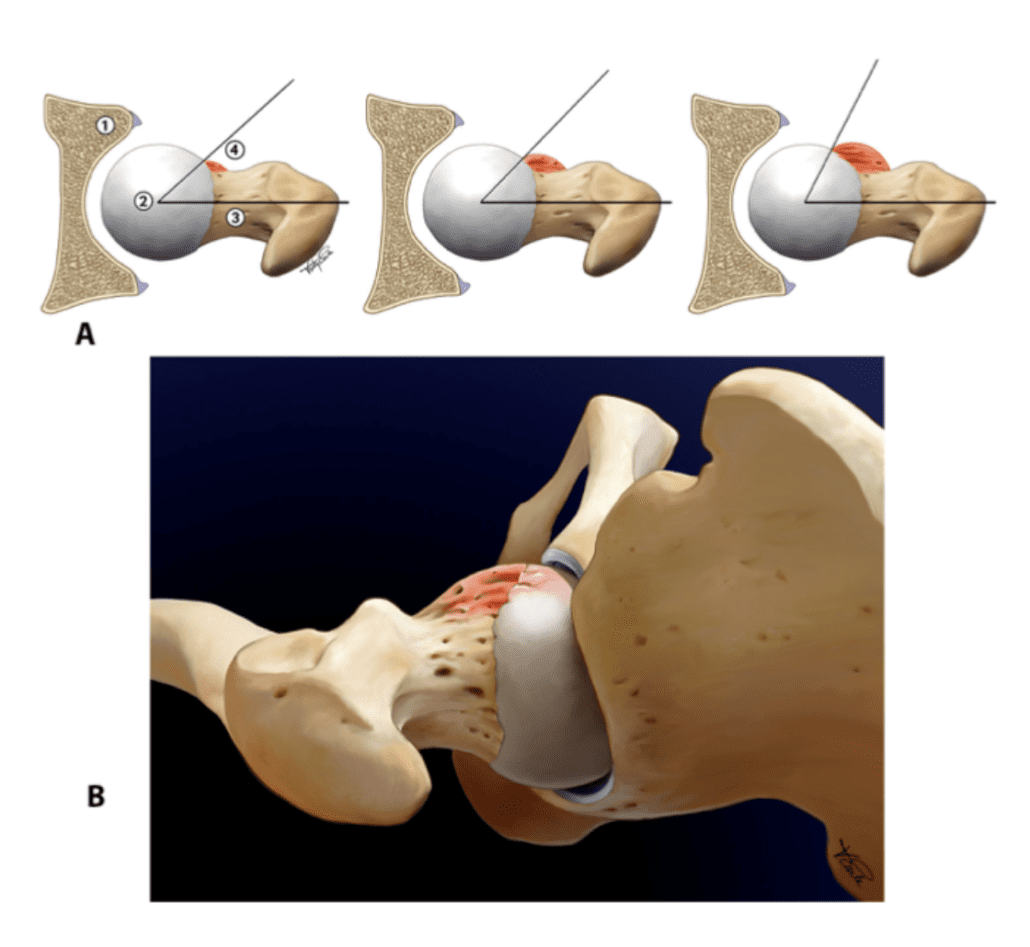
1️⃣ CAM type FAI – Morphological variation at the head neck junction of the femur (Image A)
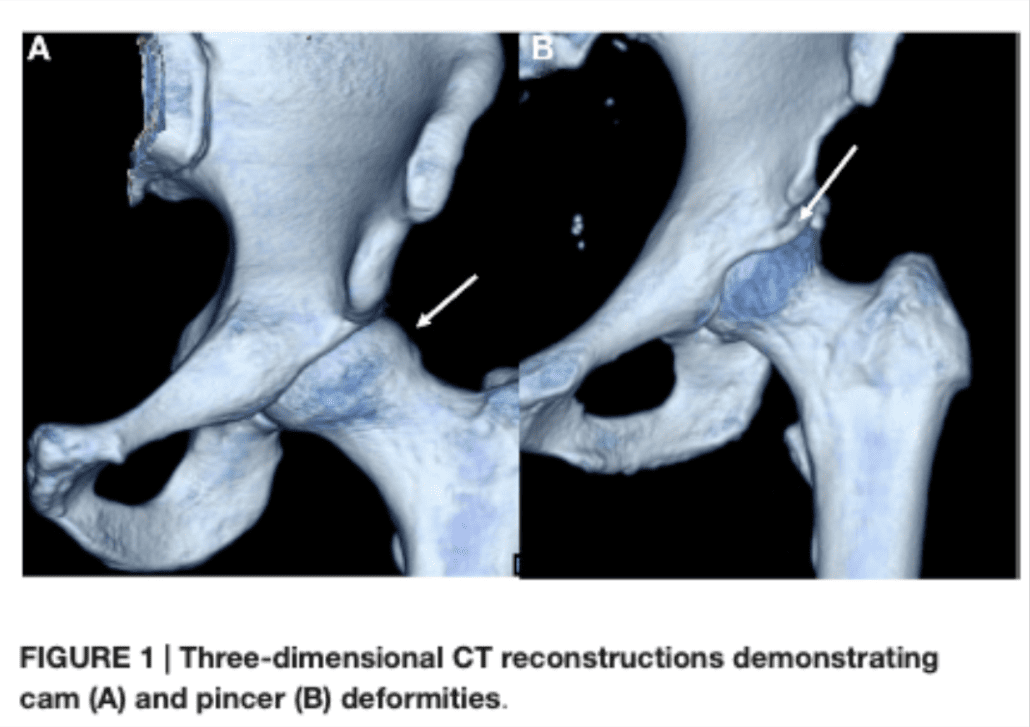
2️⃣ Pincer type – A morphological variation at the acetabular rim or bony over-coverage of the femoral head from the Acetabulum (Image B)
OR – There can be a combination of the two referred to as mixed FAI.
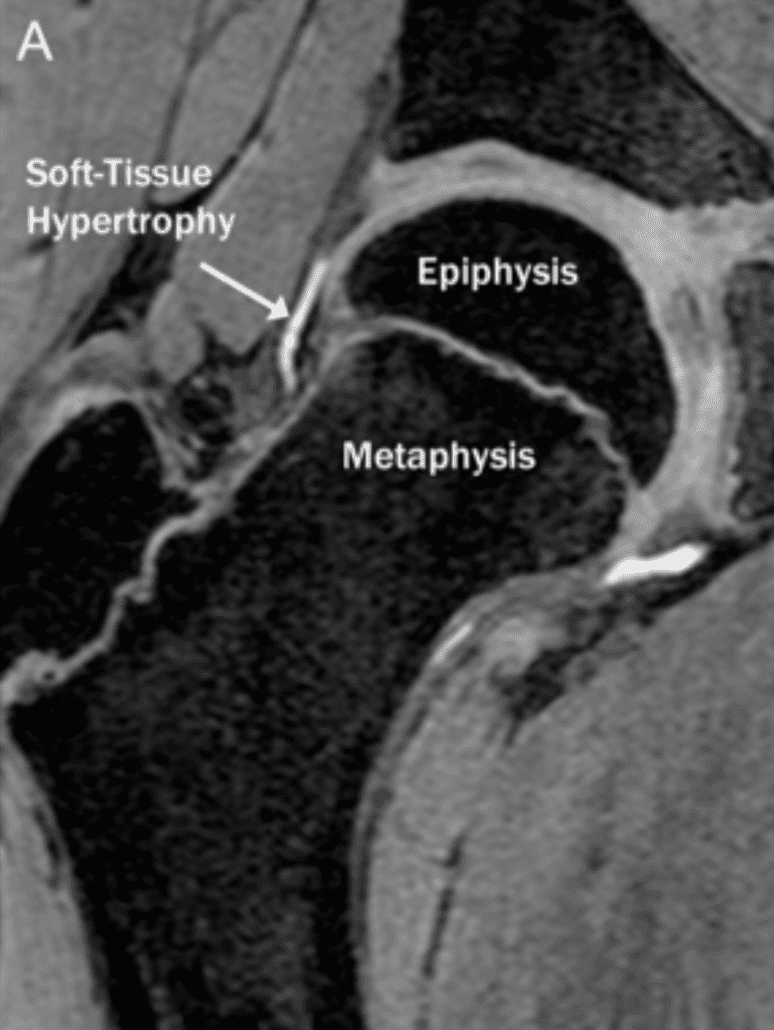
Cam type FAI development occurs between the ages of 10-14 years of age. Soft tissue hypertrophy begins at the head neck junction before the epiphyseal plate closes and then ossifies with skeletal maturation leading to a larger alpha angle.
What is an alpha angle?
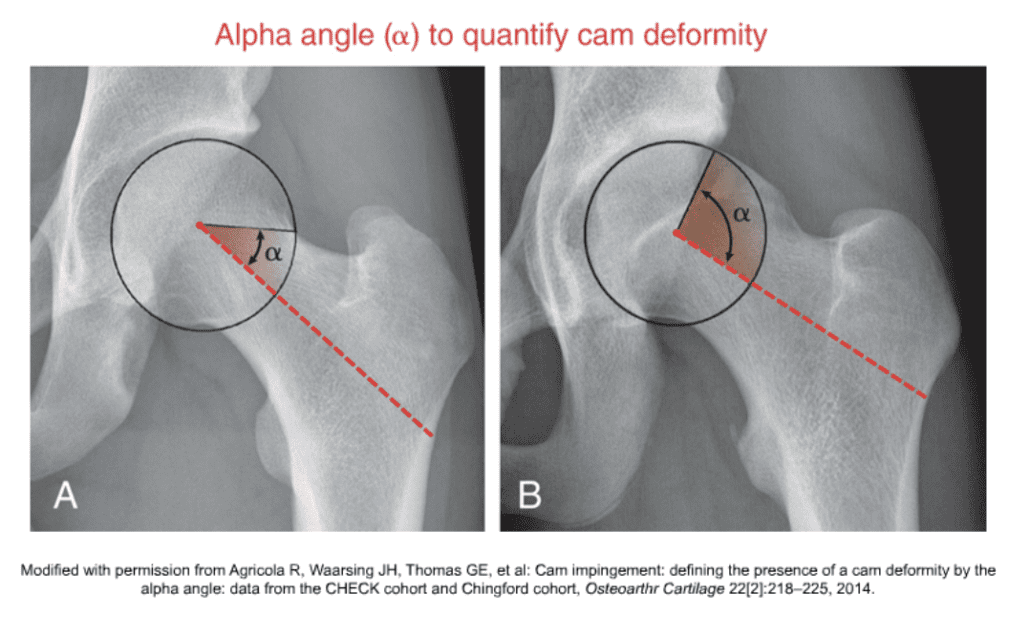
An alpha angle the degree in which the shape of the femoral head deviates from being spherical (Neumann, D 2017) In image A the femoral head is more spherical whereas in image B the femoral head is less spherical and the head neck junction is flatter.
CAM type deformity and a larger alpha angle is consistent with a higher level sport. Palmer A, et al (2018)
Males participating in competitive sport are at a greater risk of developing cam morphology and secondary hip pathology (such as labral tears, and osteoarthritis).
Do not mistake morphology for pathology
🔸 For a true diagnosis of FAI, There must be combination of symptoms, clinical signs AND imaging findings
🔸 There is often variation in the location nature, radiation, severity and precipitating factors that characterise this pain (Griffin DR, Dickenson EJ, O’Donnell J, et al 2016)
There is however also a high prevalence of CAM type deformity in the asymptomatic population.
What are the signs and symptoms?
🔸 Presents with Px in the anterior and medial hip & groin –> C sign
🔸 Deep seated ache with prolonged hip flexion / sitting in low chairs
🔸 Sharp catching / giving way pain
🔸 Painful putting on shoes and socks
🔸 Pain (in the hip and groin) getting in and out of a car
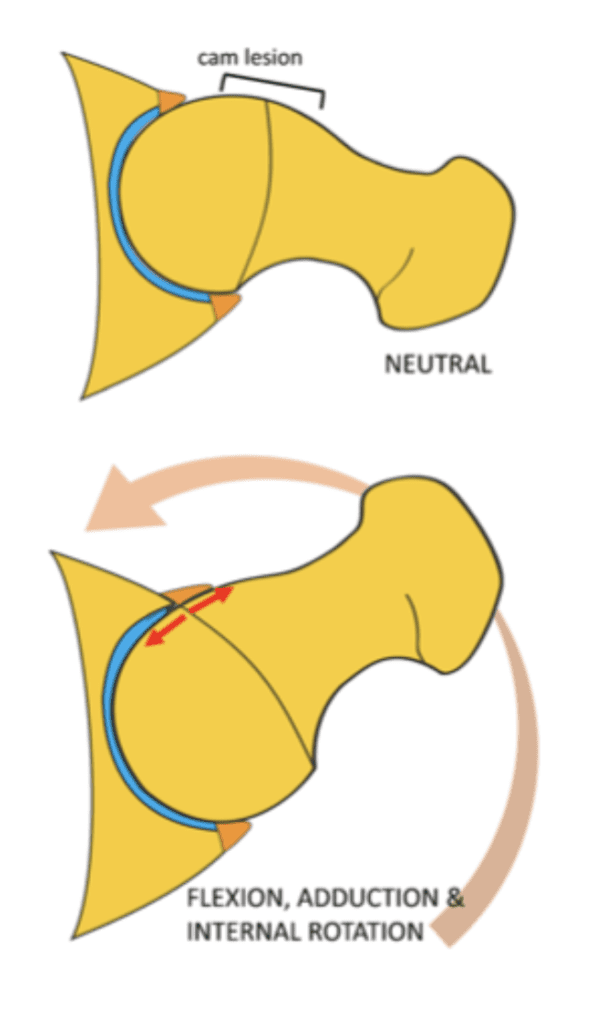
🔸 Worse with hip flexion, adduction and internal rotation (FADIR)
🔸 Often exacerbated after repetitive exercise
🔸 Hip flexion based activities aggravate such as squats, lunges, stair climbing, hill walking, running and kicking.
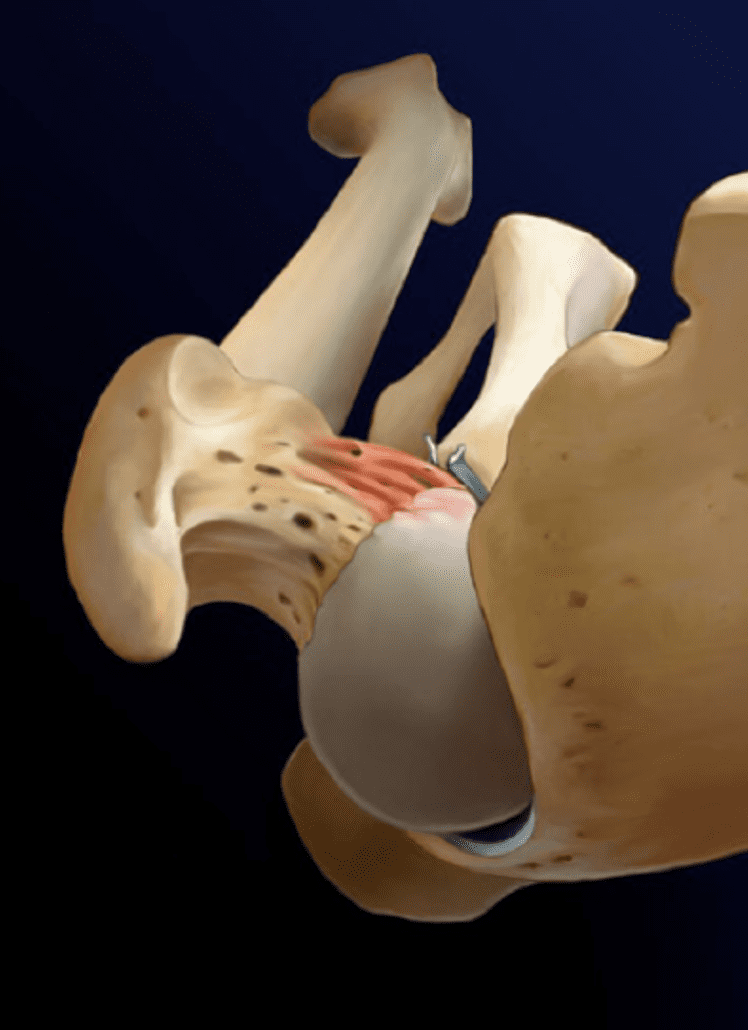
In the sporting and athletic population, Cam deformity consistently shows an association with hip pain, limited internal rotation, labral tears, chondral lesions, and ultimately hip OA (Agricola, R et al 2014) Furthermore, Hip joint pain should always be considered as a possible cause of groin pain.
Once again, It is important to differentiate morphology from pathology. Simply having a CAM or pincer type morphology does not constitute pathology or a diagnosis for FAI.
When assessing hip pain in the young and middle-age active adults, it is important to be aware of the possible continuum of hip pathology. A history of high-level sport, a high-volume of repetitive end range loading, motion related pain and limited hip internal rotation may be signs of FAI.
Labral tears often coexist with FAI as a secondary pathology. Patients with labral tears are 40% more likely to have co-existing chondropathy which leads to reduced ability to maintain a synovial seal and provide joint nutrition. (Agricola et al. 2014)
Prevalence of cam deformity is as high as 89% in athletes participating in activities that result in impact loading of the hip as compared to only 9% in non-athletic controls. (Nepple JJ. Et al 2015)
A -ve FADIR test us helpful in ruling out FAI as a diagnosis (Reiman et al 2018) due to its high sensitivity but it is not useful for ruling it in due to its low specificity.
Appropriate early detection and management is key. Management should focus on activity & load modification, progressive outcome based improvements.
Yours in Health,
Bodine Ledden



