The broken record of clinical practice
Back pain and imaging findings such as disc herniations are common in clinical practice, with lower back pain having the highest prevalence of musculoskeletal conditions worldwide. Being treated as an epidemic and the likelihood for most individuals to experience an episode in their lifetime, there’s little wonder of why poor understanding is common and misinformation can spread so easily.
Limited understanding of synovial joints and lay descriptions of discs may play part in how often we hear the phrase ‘I have a slipped disc.’
Hearing this from friends and family may lead the someone to believe that a disc is a free-floating structure, maybe a piece of cartilage that sits between two vertebrae with these alternating to form our vertebral column. It’s certainly going to contribute to the common thought that ‘If I bend too far one way, my disc might slip out the other side since it’s a free-floating cushion!’
To gain a better understanding of the grades and pathophysiology of disc herniations, consider the anatomy, first.
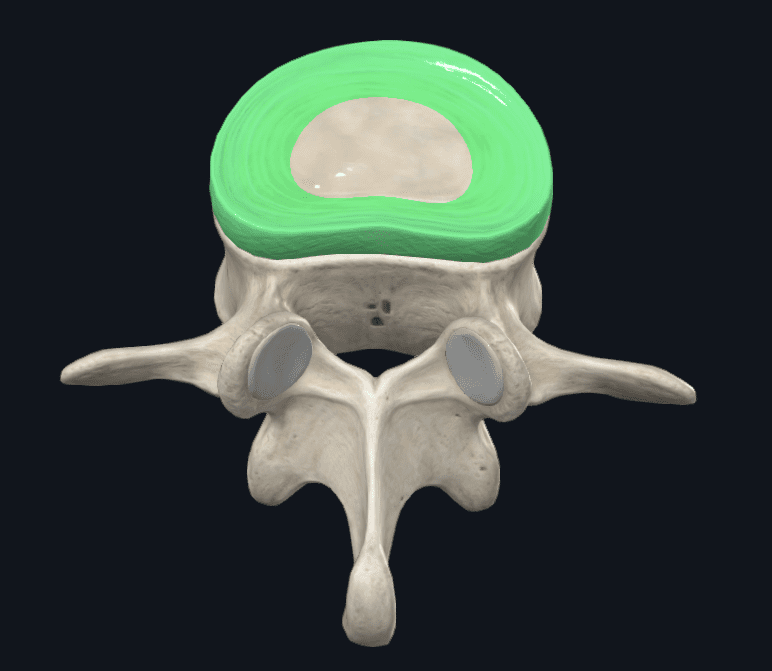
Figure 1 Lumbar Vertebra and disc (Anulus Fibrosus highlighted)
Intervertebral discs are made of three components – the anulus fibrosus, nucleus pulposus, and cartilaginous end plates.
The anulus fibrosus is formed of two layers. Both of these are composed of obliquely arranged collagen fibres. There are 15 to 25 layers arranged in alternating directions, and this increases the strength and resistance of the structure. The outer layers are mostly type I collagen fibres – the type that accounts for most of the collagen in our body – and this provides greater tensile strength due to the thick, organised arrangement of the fibres.
The inner layers of the anulus fibrosus blends throughout the concentric layers to begin containing more fibrocartilaginous (type II collagen) tissue and proteoglycan content. This allows greater flexibility and movement, whilst still providing the circumferential support that is required by the structure.
Contained within the anulus fibrosus is the nucleus pulposus. This is a gelatinous structure and rich in proteoglycans, giving it a high-water content of 70 to 80% of its wet weight. It functions to resist the compressive axial forces experienced and spreads it radially. The composition of the nucleus pulposus allows for water to be drawn in, allowing ongoing management and adaptation to the external compressive forces.
The outward spread of the nucleus pulposus due to compressive force is contained by the anulus fibrosus, in a mechanism termed ‘hoop stress’.
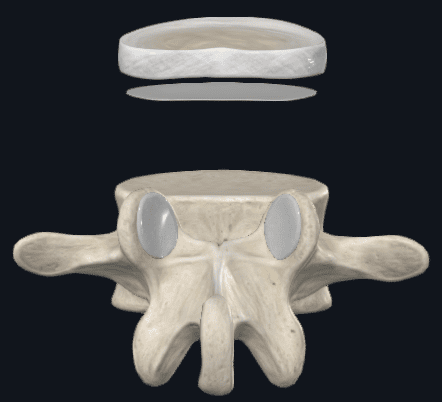
Figure 2 Anulus fibrosus and nucleus pulposus, vertebral endplate, and lumbar vertebra
Figure two shows the anulus fibrosus and inner, nucleus pulposus with the inferior vertebral endplate, and a lumbar vertebra. Missing, is a superior vertebral endplate. The endplates function to maintain the fluid pressure of the nucleus pulposus and any loss to the vertebral bodies. This is a bi-layered structure, again, of alternating directions.
The intervertebral discs attach directly to the vertebral bodies via the cartilaginous end plates, and the anulus fibrosus to the annular epiphyses (the smooth outer lip of the vertebral bodies) both superiorly and inferiorly.
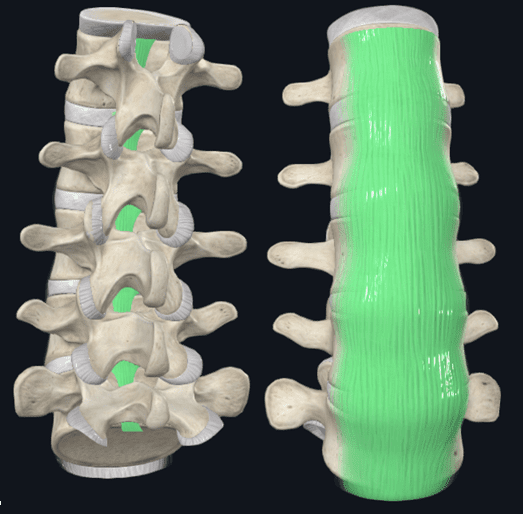
Figure 3 Posterior Longitudinal Ligament (Left) and Anterior Longitudinal Ligament (Right)
The intervertebral discs are then further supported posteriorly and anteriorly by longitudinal ligaments. These ligaments limit hyper flexion and hyper extension of the vertebral column respectively but also provides reinforcement and thickening of the anulus fibrosus.
A sound anatomical understanding of the intervertebral discs provided to patients who have experienced – or are concerned about – disc herniation provides reassurance to the strength and resilience of these structures. The terminology and depth into the topic should be adjusted for each individual’s comprehension. Questioning their understanding of the structure helps inform and correct any misunderstandings and assumptions held. Without an understanding of the relevant anatomy, it makes it difficult to address any further misunderstandings and negative beliefs and provide a more reassuring model.
Addressing the broken record –
A ‘slipped disc’ is the incorrect terminology for disc herniation, and there are several grades of disc herniation.
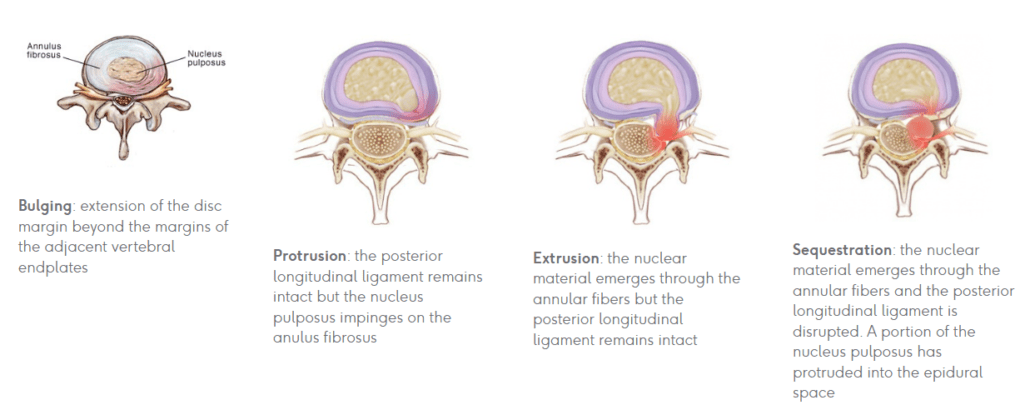
Figure 4 Stages of Disc Herniation (I – IV)
Understanding each grade is shared in figure 4.
It’s important to note that the four stages of disc herniation commonly present in asymptomatic individuals and symptoms will usually resolve in a matter of weeks (Brinjikji et al. 2015, Stretanski et al. 2025).
These findings may be present for some months and whilst they are a factor in back pain, painful episodes with imaging revealing a disc herniation should consider these as a piece of the puzzle, instead of the sole reasoning or ‘root cause’ to the issue.
Chiu and colleagues (2015) found in their systemic review that the rate of spontaneous regression for disc herniations was greater for higher grades of disc herniation. It was found that disc sequestrations saw a 96% regression, disc extrusion had 70%, disc protrusion found 41%, and 13% for disc bulging presentations.
There is a greater autoimmune response with a foreign body being recognised and increased macrophage activity in disc sequestrations, which would account for the higher rates of regression the higher the grade of herniation.
Appropriate loading through volume and frequency modulation has shown improvements in disc adaptation. Approaching load with a high intensity, low volume, and low frequency had been shown to improve disc adaption and regression (Chan et al. 2011, Steele et al. 2015).
Among other mechanisms, the authors also suggest that the compression and decompression of intervertebral discs act to squeeze out water, bioactive factors and metabolic waste, then allow fluid return after compression is reduced. Chan and colleagues reported that there is a 20-25% expression and reabsorption of water content through this process.
These facts of the asymptomatic presence of disc herniations, spontaneous resorption, adaptive resilience, and the robust anatomy of the vertebral column and intervertebral discs are all positive education points to share with patients who may be misinformed and concerned of potential disc herniations.
This should be done to address any negative beliefs about back pain and allow for return to their activities of daily living, reintroduction of load, and the freedom to explore movements after pain onset.
Questioning your patients understanding, or asking them to describe a disc herniation will help reveal where the divergence in understanding lies, and where best to focus your attention alongside any other treatment interventions implemented.
