I have Sciatica…

What does that even mean?!
Sciatica is a symptom that may be originating from a plethora of pathophysiological causes.
Firstly, we should consider that the layman may understand sciatica as ANY pain that is referred into the leg, and Dr Google will often (unfortunately) confirm their suspicion of this…
When a patient presents to your clinic with a diagnosis of sciatica, it is important that we investigate much further to identify the cause of these symptoms.
Where do we start?
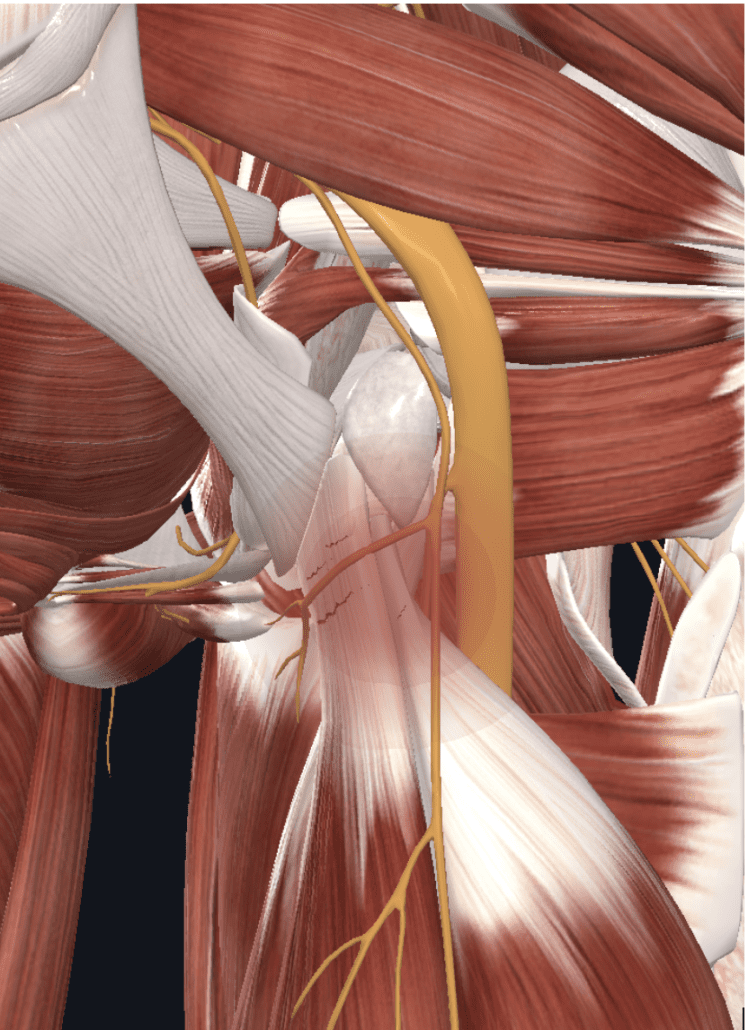
Sciatica is a symptom of compression, chemical irritation, stretch, crush injuries or even transection to the sciatic nerve. This can range from focal segmental demyelination of a nerve (damage to the protective connective tissue coating around the nerve), from neuropraxia, through to it being completely severed (usually from iatrogenic causes).
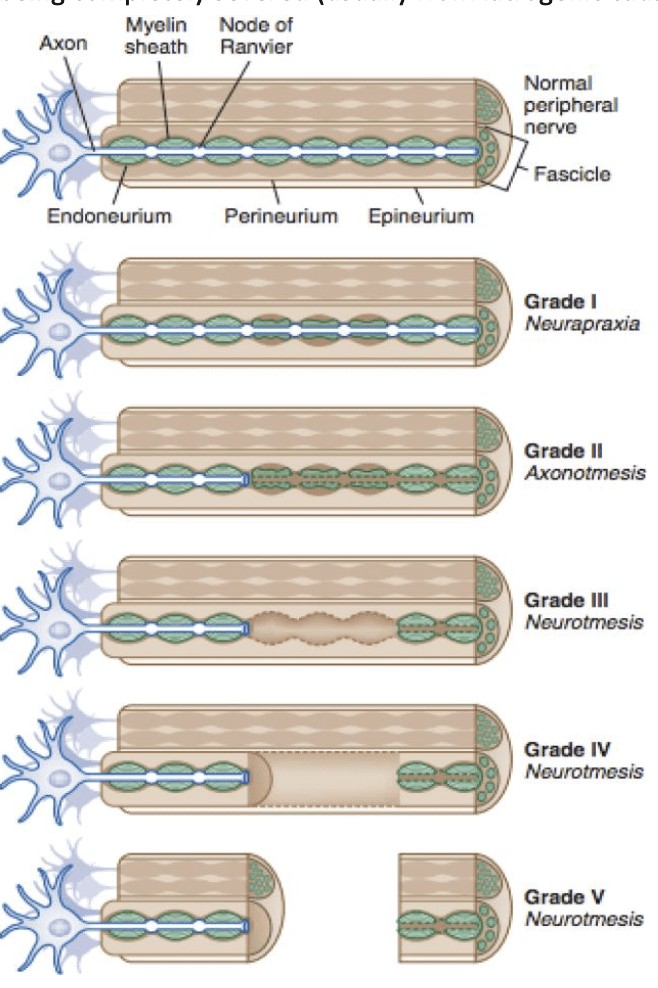
With the most common type of nerve injury being compression. This often occurs from bone or soft tissue compression, or external forces. (Neuropraxia as pictured above).
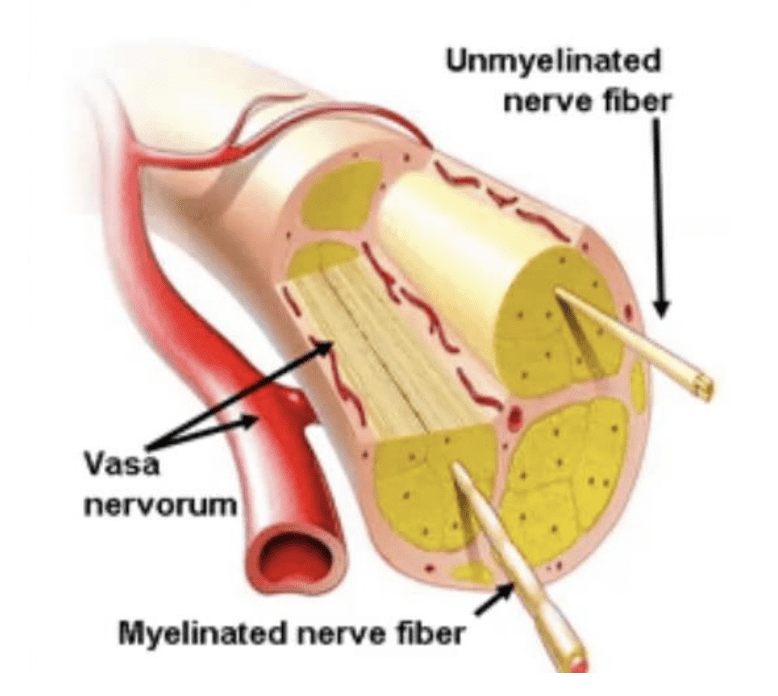
Nerves are very blood thirsty (you may have noticed that there is usually major nerves arteries and veins travelling together) hence these structures do not like to be compressed as this limits their oxygen, blood and impairs conductivity.
The nervous system takes in 20% of our total oxygen consumption, delivered to the nerves by small arteries called the vasa nervorum. Think of those times when you slept with your arm over your head and woke up with a dead arm. You wake up and move it around, clench your fist a few times to get some more blood flow into the area and it recovers quickly. However long-term nerve compression can have more significant implications.
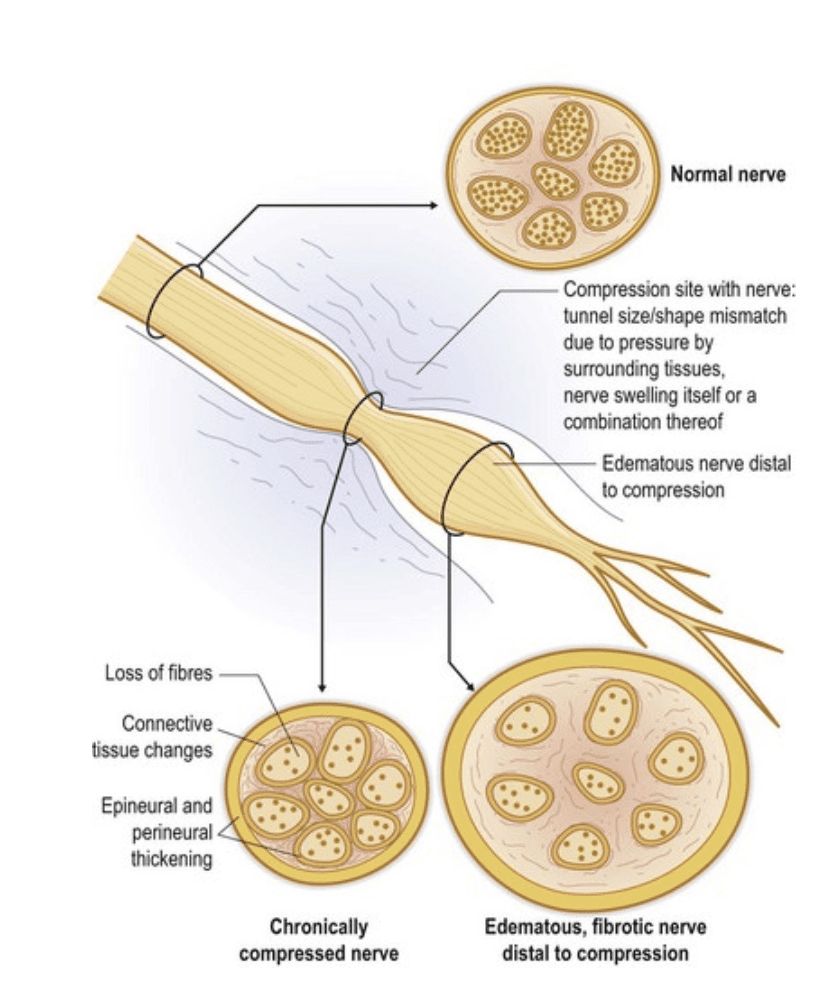
If blood supply to a nerve is impaired this leads to decreased oxygen supply. This compression over an extended period can lead to fibrosis that can impair the nerve’s ability to slide in relation to surrounding tissues. These irreversible fibrotic changes can lead to demyelination and a loss of conduction of the nerve.
But why is it so painful?
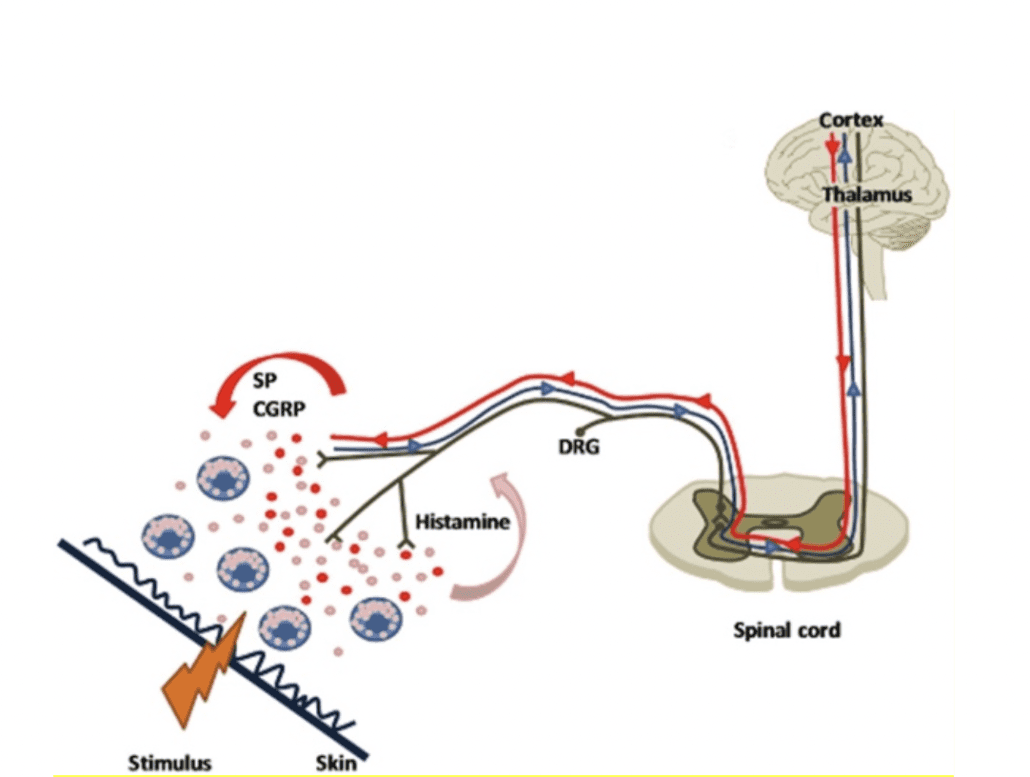
When a nerve is compressed, irritated or damaged, it can lead to neurogenic inflammation. A process where inflammatory chemicals are released via antidromic impulses (this is inflammatory chemicals sent in the opposite direction to the normal direction of that nerve).
These chemicals include Substance P (SP) & Calcitonin Gene Related Peptide (CGRP). This can lead to a lowered nociceptor threshold leading to increased sensitivity and upregulation of the nerve activity.
Now that we understand that nerves get cranky when they are compressed, Lets have look at the anatomy of the sciatic nerve.
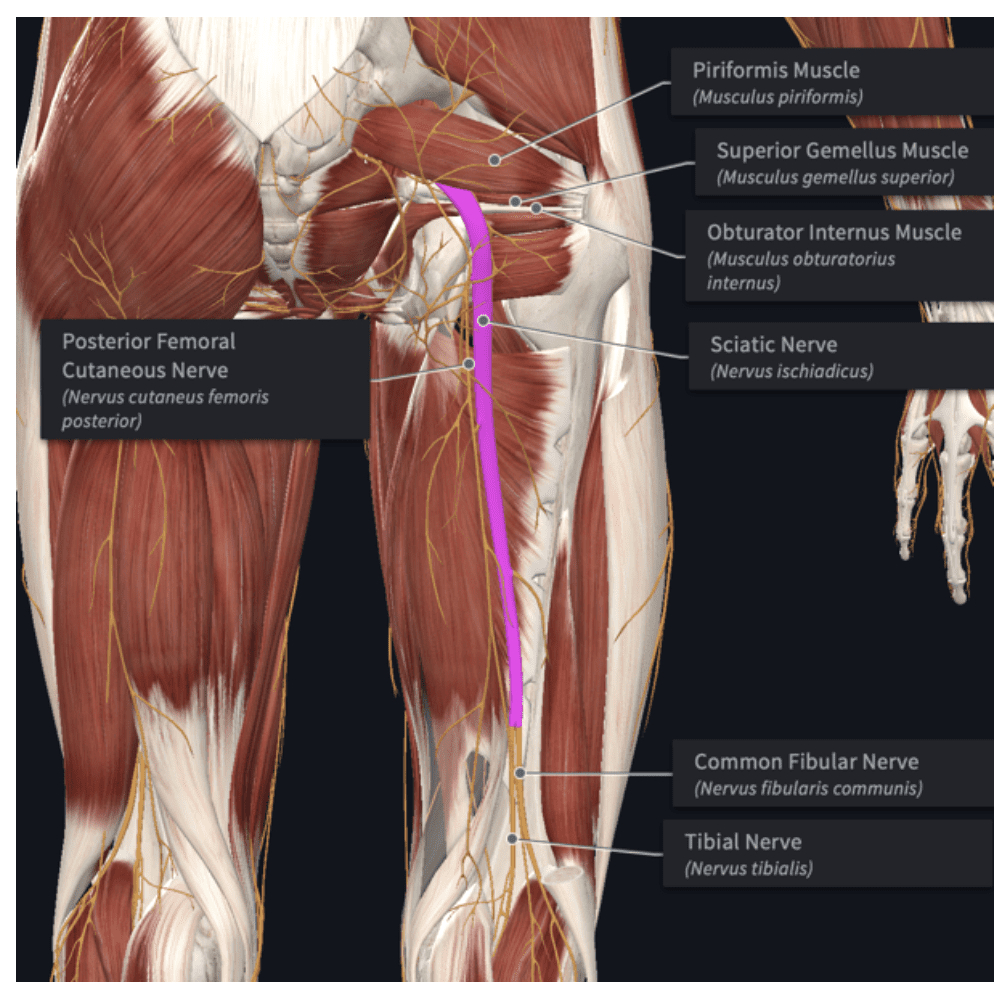
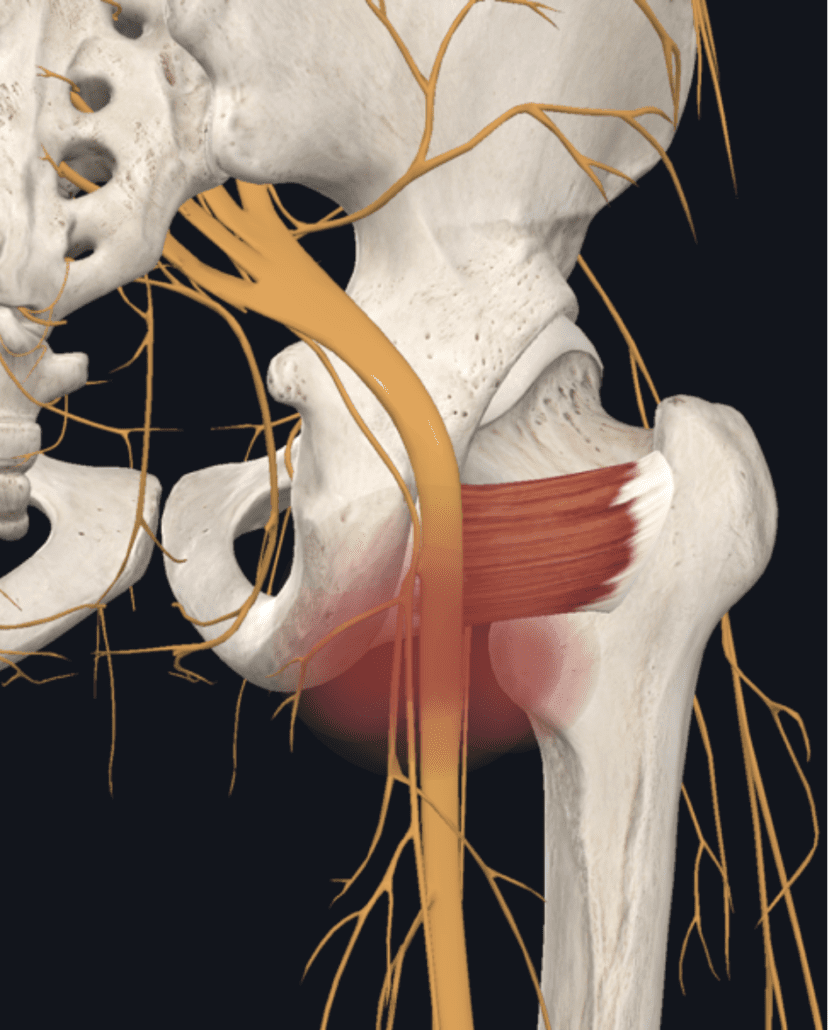
The sciatic nerve originates from L4-S3 nerve roots. It then passes through the greater sciatic notch beneath the piriformis through the deep gluteal space, lateral to the ischial tuberosity. Here the sciatic nerve gives rise to the muscular branch of the sciatic nerve that provides motor innervation to the hamstrings and the hamstring fibres of the adductor magnus.
The sciatic nerve continues to travel down the posterior compartment of the thigh deep to long head of the biceps femoris and superficial to adductor magnus and short head of biceps femoris.
It branches into the tibial nerve and common fibula nerve just before the popliteal fossa passing into the lower leg and further branching to provide sensory any motor innervation into the lower leg.
Why did I tell you all of this?
Well, this nerve can be compressed / trapped / over stretched or irritated anywhere along its interface, which may lead to sensory or motor changes along the distribution of the nerve. So again, we need to ask more questions about their history.
Firstly, rule out any serious pathology including:
- Malignancy
- Tumor
- Infection
- Systemic inflammatory disorder
Do they have:
- Pain that is increased or unrelieved with rest
- Associated night pain, bone pain and morning stiffness
- Visceral pain, symptoms of claudication
- Loss of motor function
- Bowel and bladder dysfunction
- Saddle anesthesia
- Fracture
- Unexplained fever
- Unexplained weight loss
Great now that you have taken a thorough history, we then should identify if it is a Central V’s Peripheral cause of nerve irritability / sensitivity…
Central causes of nerve irritation commonly consist of:
👉 Lumbosacral disc pathologies
👉 Lumbosacral facet syndrome
👉 Lumbosacral spine sprain
👉 Lumbosacral spondylolisthesis
👉 Lumbosacral spondylolysis
👉 Sacroiliac joint injury/dysfunction
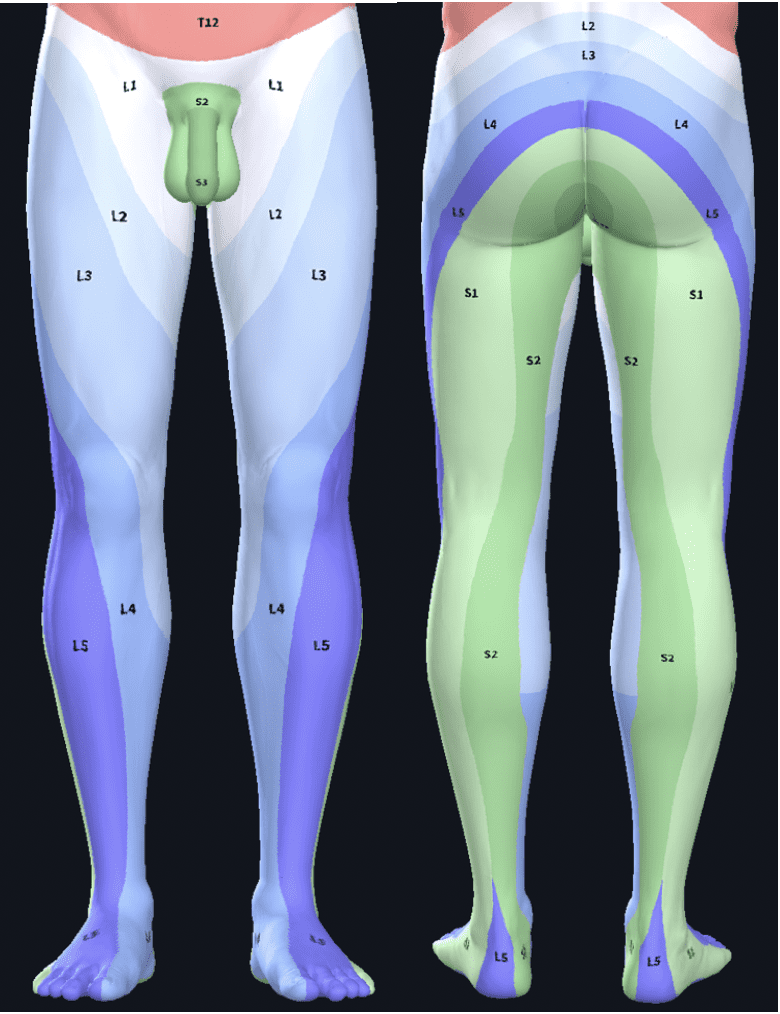
These types of pathologies typically cause compression / irritation to the nerve root which often give rise sensory changes along a dermatomal distribution.
In an acute injury (for example a lumbar disc pathology) there is likely to be an inflammatory component. This inflammatory component can increase the sensitivity of nociceptors and also sensitise the nerve leading to an increase in neural symptoms.
However, if there is compression or irritation to the motor component of the nerve there will often be signs of diminished strength / motor function and possibly atrophy.
Sounds like a lot to consider right?
Gaining a thorough history and understating the mechanism of injury is key. Identifying aggravating and easing factors, quality of pain, specific location of pain, level of irritability, history of injuries, age, level of activity, comorbidities etc can all provide you with a good idea of what may have caused or be driving the symptoms along with the severity of the condition.
Ok, you have ruled out red flags and other central causes of pathology…what’s next?
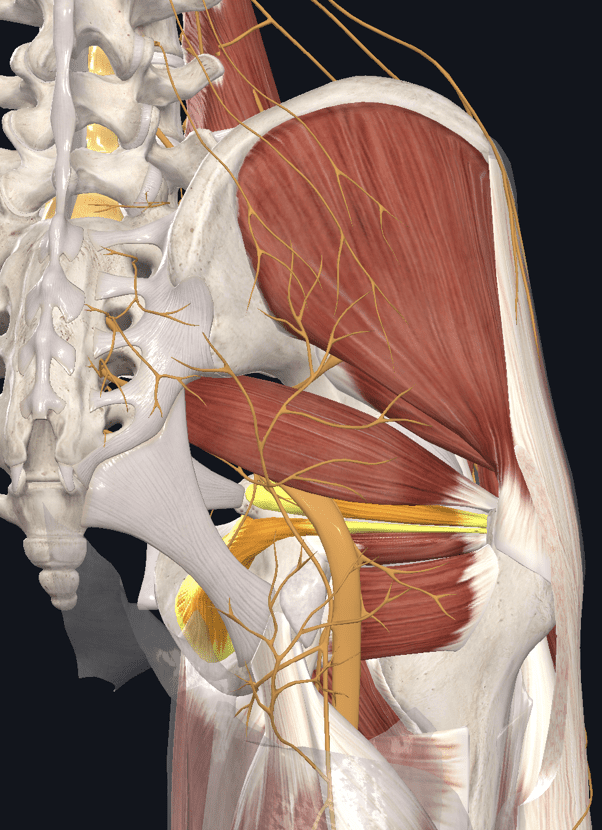
Peripheral sites of compression in the deep gluteal space (yes there is much more than just the Piriformis that can cause sciatic nerve compression in the periphery…in fact, Piriformis syndrome only occurs in 0.3-6% of all cases of low back pain and/or sciatica. (Hicks BL, 2021)
Compression in the deep gluteal space can occur as the sciatic nerve passes under the belly of the piriformis and over the Superior Gemelli/Obturator Internus, a scissor-like effect between the two muscles can be the source of entrapment. This is referred to as Gemellus/Obturator syndrome.
Irritation to the nerve may also occur as a result of chemical irritation to the nerve from other pathologies such as Ischiogluteal Bursitis, proximal hamstring tears or tendinopathy leading to secondary sensitisation of the sciatic nerve and/or posterior femoral cutaneus nerve.
It can be due to trauma from a fall or contusion that may irritate the sciatic nerve in the deep gluteal space.
Other causes may be due to prolonged compression from sitting on a wallet in the back pocket or from sitting on hard surfaces.
Less common causes of DGS include ischiofemoral impingement which is a result of the mechanical compression of the nerve between the lesser trochanter and the ischial tuberosity.
This is often activity related that is exacerbated with hip extension and adduction / long stride length. It is often relieved by hip flexion and rest.
There are several potential causes of peripheral nerve entrapment in the deep gluteal space.
The term ‘deep gluteal syndrome’ rather than “piriformis syndrome” is preferred to describe the presence of pain in the buttock caused from non-discogenic and extrapelvic entrapment of the sciatic nerve. (McCrory, P., Bell, S. 1999) (Martin, H. D et al. (2015).

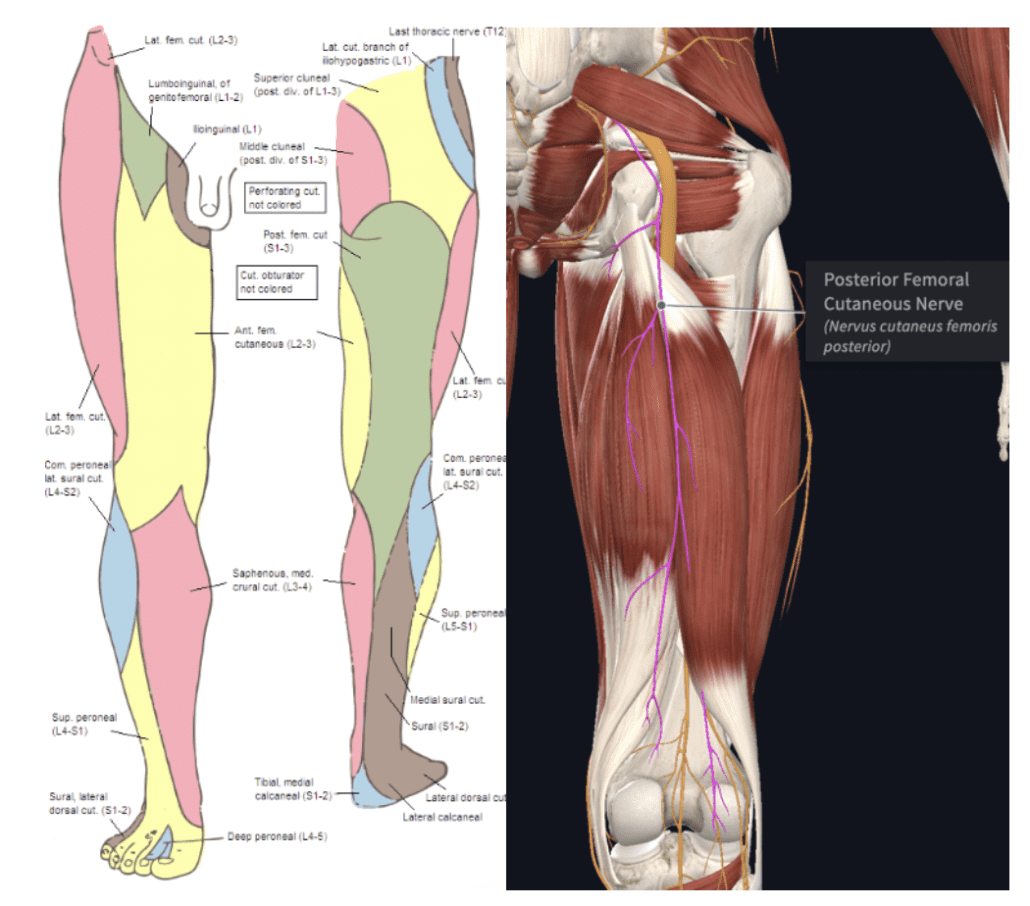
And let’s not forget about the Posterior Femoral Cutaneous Nerve (PFCN) This nerve arises from S1-S3. Passing through the greater sciatic foramen below the piriformis. It and provides sensory innervation to the posterior thigh buttocks, perineal region and popliteal fossa.
The clinical history of a peripheral (Sciatic nerve or Posterior femoral cutaneous nerve) compression may include:
👉 Previous injury
👉 Trauma from direct fall can irritate the sciatic nerve
👉 Sports involving high loads of flexion adduction and internal rotation
👉 Sitting for extended periods on hard surfaces
👉 Sitting with knees ‘kissing’ for extended periods
👉 Repeated hip abduction exercise with knee flexed at 90 deg (yes you all know this exercise from the gym right?!)
👉 Hip flexion, adduction and internal rotation can cause narrowing of the space between the inferior border of the piriformis, superior gemellus and sacrotuberous ligament.
They will often be complaining of:
👉 Buttock pain
👉 Paresthesia into the posterior thigh
👉 Altered sensation burning, tingling shooting pain
👉 Worse after sitting 20-30 minutes
👉 Sitting cross leg makes it worse
👉 Stretching hip external rotators is often provocative i.e. pigeon stretch
👉 Limping
👉 Worse at night
👉 Painful getting out of bed
👉 Altered by hip movements
👉 Tenderness over the greater sciatic notch
👉 Relieved during the day relieved with standing
WOW 😲 that’s a lot…
There is a lot to be considered when a patient describes “sciatica” like symptoms. The importance of understanding the potential pathoanatomical cause can be key to directing management.
What do we want you to take from all this?
The main thing is to understand that “Sciatica” by itself is an ineffective diagnosis.
It doesn’t provide adequate information to be able to structure an appropriate treatment plan.
The Sciatic nerve has (as you have just seen) has a very large number of factors that can negatively influence it. So when your client walks in the door saying that they have been diagnosed with Sciatica, be prepared to conduct your own assessment and ensure you have taken a deep dive into their particular presentation and all that it involves.
If you read this article and thought that there is so much here that you don’t understand or know how to do, don’t despair!
The good news is that there is a plethora of information freely available to the therapist willing to go looking, reading and asking questions.
The ACE Research Library is a great place to start, you’ll find some great relevant articles.
And never forget that truly great health professionals are always trying to learn more and stay at the top of their game.
So keep your eyes and your mind open!
Bodine Ledden.