Why do you need to know that

Do you take any recreational or performance enhancing substances?
These are questions that would sound quite fitting to a police interview room, or maybe an attorney’s line of questioning of a witness. But they’re also on most allied health professional’s intake forms.
These are very personal and intrusive questions to ask a stranger. We then might go further and ask questions like medical or cognitive diagnosis’, any altered sensation of the saddle region, or incontinence issues. Some of these are to identify red flags, relevant for specific presentations. Broadly, these provide beneficial information for most cases.
A patient may very rightly ask what the importance of these lifestyle questions are, so it’s important that we understand why they’re so commonly included on intake forms and history taking, and how we apply this knowledge into a treatment plan.
First, consider the factors of a painful presentation –
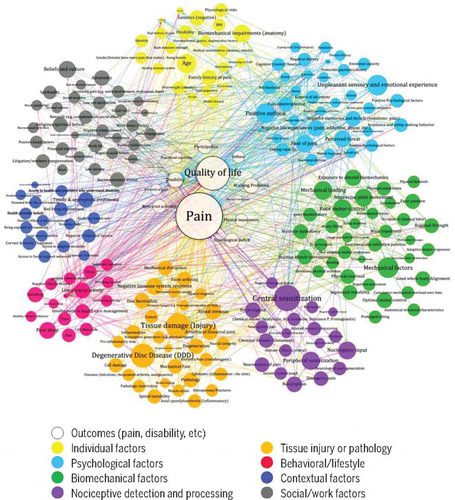
Figure 1 – Cholewicki et al. 2019
In the middle of this map are the outcomes of lower back pain; the more tangible qualities that the patient experiences. Various factors are colour coded and links shown of their interactions with each other. These are the usually intangible factors that we measure through assessment, imaging, or questioning.
If we consider just the outcomes of a patient’s lower back pain experience, there’s much more than what is commonly the sole focus of most patients and some clinicians –
Pain
Instead of pain being a straightforward result of an injury or accident, it’s the outcome after we consider each one of these factors and how they may contribute to the outcome of pain. This is impacted in varying degrees or links between factors for individuals.
Lifestyle questions that cover factors such as diet, nutritional intake, sleep quality, social or recreational activities are extremely important. These provide an understanding of potential tissue changes through nutrition, psychological stress through sleep and regulation whilst engaging in hobbies and experiencing social support.
Jain et al. 2024 reported that sleep impairment was a stronger predictor for chronic pain than chronic pain being a predictor of sleep impairment.
The International Association for the Study of Pain (IASP) define pain to be
An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage
Pain, being a sensory and emotional experience, is very likely then to have a greater impact on those patients that we identify to have greater emotional impacts through screening, such as emotional or cognitive disorders, reduced social engagement and participation, or a low social support network.
Another question commonly asked during intake is of a patient’s occupation. This not only provides another insight into the impacts to sleep quality, stress, and work-life balance, but also socioeconomic factors.
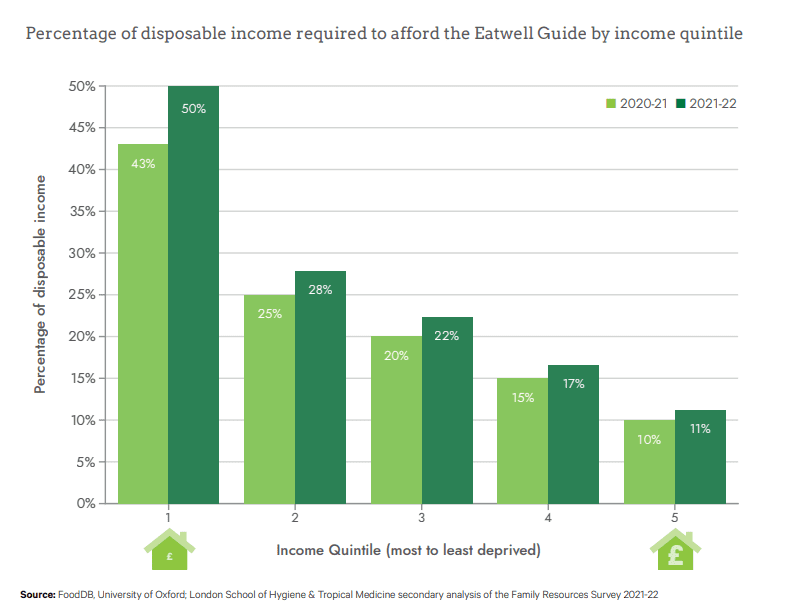
Figure 2 – The Broken Plate 2023
Moreover, socioeconomic status also presents as a risk to chronic pain, as well as postoperative pain and pain management as discussed in a meta-analysis and systematic review by Prego-Dominguez et al. 2021 and Thurston et al. 2023, respectively.
Throughout these and similar articles, other factors that are commonly highlighted for pain and pain management are smoking, history of depressive or anxiety symptoms, and sleep difficulties. All questions that are important to include and follow up with when completing a thorough history.
A rather difficult conversation, but one that is important in pain management is an individual’s use of recreational or performance enhancing substances (PES). PES such as anabolic-androgenous steroids are well documented to have increased risk of tendon degeneration, pain, or possibly rupture as muscle hypertrophy may occur at a rate faster than tendon adaptation (Pope et al. 2013 and Zywiec et al. 2025).
Recreational substances are often used in the self-management of pain, with increased risk alongside the use of PES through the partaking of high-risk taking behaviour, pain management, and susceptibility to opioid dependencies reported by Avary and Pope 2000 and Zywiec et al. 2025.
Recreational substance use may act as an alternative management of pain, anxiety or depressive symptoms for patients. The impact created is that tolerance of the substances may increase in time, leading to greater use and dependency of the substance. There is also the progression of use of other substances alone or in combination.
Masking of these symptoms can lead to poor adherence to treatment plans, return to ADLs, sports, or occupation, furthering risks and impacts associated with pain and injury. There are also further social impacts for individuals, with social support, engagement, and participation impacted through lifestyle changes.
One of the larger factors of pain outcomes shown in Figure 1 is central sensitisation (CS). The IASP, described CS as
Increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input.
A key component in CS is continued noxious bombardment of afferent pathways to a spinal segment, leading to allodynia and hyperalgesia of the tissue represented by this spinal segment (homosynaptic representation). This may cross to impact the contralateral, superior or inferior segments (heterosynaptic representation) impacting the tissue represented in multiple spinal segments, expanding the receptive field.
Clinical features of CS reported by Dydyk et al. 2025 include more than just continued noxious bombardment. CS is frequently associated with mood and sleep disturbances, fatigue, cognitive impairment, and pain catastrophizing.
This highlights the importance of a thorough and varied questioning throughout the patient intake and history for presentations of chronic or widespread pain especially. Asking these questions for acute pain or injury caused by clear mechanism of injuries is still of great importance. Early identification of these clinical features is beneficial in treatment, management, or referral for individuals that may be experiencing factors concurrent with CS during early pain onset, rather than the progression of symptoms and pain, potentially leading to CS presentations.
Whilst conversations can be difficult and a strong therapeutic alliance greatly benefits approaching these factors highlighted, a sound understanding of the reasoning that these factors are asked throughout the process will help to identify if there are common trends that may be brought up in a later session, once rapport and trust has been established.
